
Uma Maheswari K¹, Renuka Devi MR²
¹Final Year Post-Graduate, ²Professor and HOD Department of Physiology,
Sree Balaji Medical College and Hospital, Chromepet, Chennai, Tamil Nadu, India
Abstract
Background: Diabetes Mellitus (DM), a clinical syndrome characterised by an increase in blood glucose concentration. Hyperglycemia induces changes in the platelet function in Diabetes Mellitus subjects. Platelet Indices include parameters such as mean platelet volume (MPV), platelet distribution width (PDW) and plateletcrit (PCT).
Aim: To study the platelet indices in Diabetic Mellitus subjects, to compare the platelet indices in controlled with uncontrolled Diabetes Mellitus, to compare the platelet indices in Diabetes Mellitus with normal subjects.
Materials and methods: A cross – sectional study was conducted in (100 – Diabetes Mellitus & 100 Control(normal) subjects. Written Informed consent was obtained from the subjects. Each subject was asked to fill up the questionnaire on history of Diabetes Mellitus and general information. Blood parameters like Platelet Count, Mean Platelet Volume, Platelet Distribution Width, Plateletcrit, Fasting Blood Sugar, Post-Prandial Blood Sugar, HbA1c were estimated.
Results: Among the Diabetic group, the FBS, PPBS and HbA1c was higher in uncontrolled DM than in DM subject under glycemic control, which was statistically significant. Platelet indices showed statistically significant difference between controlled and uncontrolled DM. MPV and PDW showed statistically significant difference between Diabetic and control group. Plateletcrit was not different between Diabetic and control group. Conclusion : Our study found that hyperglycemia leads to platelet hyperactivity. The control of glycemic status in each and every Diabetic individual can prevent the development of micro vascular and macro vascular complications.
Keywords: Diabetes Mellitus, Mean Platelet Volume, Platelet Distribution Width, Plateletcrit.
Corresponding Author ::
Dr. K. Uma Maheswari,
Department of Physiology,
Sri Balaji Medical College,
Chrompet, Chennnai.
96, M.R Nagar, Second Main Road,
Kodungaiyur, Chennai – 600 118
Telephone: +91 9677125359
E-mail: [email protected]
Introduction: Platelets are non – nucleated, colourless, disc shaped and smallest blood cells of diameter(2 – 4 μm) derived from megakaryocytes and found in bone marrow.1 The normal range of platelet count is 1,50,000 to 3,00,000 lakh / microliter.2 Platelet Indices includes parameters such as plateletcrit, mean platelet volume and platelet distribution width. The mean platelet volume (MPV) is an index of the average size of platelets in blood and a marker for assessing platelet function and activation.3 Platelet distribution width (PDW) reflects uniformity of the platelet size. PDW is a simple and specific marker of platelet activation. Plateletcrit (PCT) measures the total platelet mass. PCT is related to the platelet count and size of the platelets.MPV and PDW shows the reflection in the variation of size in the circulating platelets.4 PDW and PCT is important in assessing tendency for atherosclerosis and thrombosis.
Diabetes Mellitus (DM) is a clinical syndrome characterised by hyperglycemia, polyuria, polydipsia, polyphagia, weight loss and tiredness. Diabetes Mellitus is associated with microvascular and macrovascular complications. These complications are the major cause of morbidity, mortality and decrease in quality of life.
In 2010, prevalence of Diabetes was 6.4% and by 2030, it is expected to rise to 7.7% worldwide. In India, the prevalence of Diabetes is slightly higher than the world average (9.1%vs.8.3% worldwide). In India, the number of Diabetes Mellitus cases in 2030 is expected to increase from 50.8 million to 87 million.7 Diabetes Mellitus is considered as a prothrombotic state with increased activation of platelet.8 The development of chronic complication has a close relationship to platelet dysfunction. Hyperglycemia, insulin deficiency, insulin resistance, metabolic condition, and cellular abnormalities in Diabetic patients.
Aim: To study the platelet indices in Diabetic Mellitus subjects.
Objectives
• To compare the platelet indices in controlled with uncontrolled Diabetes
Mellitus
• To compare the platelet indices in Diabetes Mellitus with normal
subjects.
Materials and methods: A cross – sectional study was conducted among 100 Diabetes Mellitus and 100 normal (control) subjects who were attending the Endocrinology and General Medicine Department in Sree Balaji Medical College & Hospital, Chromepet. Subjects of both genders was recruited for this study. The study was approved by the Institutional Ethical Committee for human research The procedure and purpose of the study was clearly explained in detail to the subjects. Written Informed consent was obtained from the subjects in their own language. History regarding duration of the disease, treatment regimen, presenting complaint, past history, socioeconomic status and family history of Diabetes Mellitus were collected.
Inclusion criteria
• Age group – 25 to 70 years
• Both male and female gender
• Healthy volunteers with no medical illness (control group).
• All known cases and newly diagnosed Type 1 and 2 Diabetes Mellitus.
• The subject on oral hypoglycemic drugs were included.
Exclusion criteria
• Smokers
• Subjects with Congenital or acquired platelet disease,
• Subjects on antiplatelet and anticoagulant therapy.
• Individuals with hypertension, renal failure, heart disease, stroke,
liver disease and other systemic illness are excluded from the study.
After an overnight fasting, around 5 ml venous blood was collected from all the subjects.Blood parameters like Platelet Count (PLT CT), Mean Platelet Volume (MPV), Platelet Distribution Width(PDW), Plateletcrit (PCT), Fasting Blood Sugar (FBS), Post-Prandial Blood Sugar (PPBS), HbA1c were estimated. Data was collected, entered in Microsoft Excel, expressed as mean ± SD (standard deviation) and analysed by using independent samples test in SPSS version 20.
Results: 100 subjects with Diabetes Mellitus (DM) and 100 normal (control) were enrolled for this study. There were 62 males and 38 females in Diabetic subjects group. The Diabetic group was divided into controlled and uncontrolled DM. In a controlled group of 50 Diabetic patients, 32 subjects were males and 18 subjects were females. In Uncontrolled group of 50 Diabetic patients, 30 subjects were males and 20 subjects were females.
Discussion: Platelet plays an important role in maintaining the normal haemostasis. Changes in platelet morphology and its functions have been reported in Diabetes Mellitus. Altered platelets morphology in Diabetes Mellitus is associated with an increase in risk of developing vascular complications.
In our study, there is no statistical significance in mean age and sex of controlled Diabetes Mellitus and uncontrolled Diabetes Mellitus. This means our findings were not influenced by age and sex. Similar to our study, there were no significant difference of age and sex of the Diabetic and non- Diabetic subjects in these studies.10-12 The Body mass index is higher in Diabetic group than the non – Diabetic group. This result is similar to Biswal et al study.
Therefore, in our study, the sample chosen were matched with respect to the anthropometric data between the two Diabetic groups. In our study, the mean FBS, PPBS and HbA1c of uncontrolled Diabetes was higher when compared to the controlled Diabetes group. There is a statistically significant difference between the two Diabetic groups. Similar to the study done by Yenigün et al.12
The mean value of HbA1c in my study is 7.47 ± 1.74%. The glycemic status of uncontrolled Diabetes was higher (8.85 ± 1.42%) when compared to the controlled Diabetes group.13 When compared with normal subjects, the Diabetes Mellitus subject had values that were significantly higher. Similar findings were found in other studies.14-17 The platelet count in controlled DM group (2.69 ± 0.60lakh/cu.mm) was lower than that of uncontrolled DM group (2.97±0.81lakh/cu.mm), but was not statistically significant (p=0.058). When compared to the controls (2.49 ± 0.74lakh/cu.mm), the platelet count was higher in Diabetes. This result was compatible to the results of Swaminathan et al., Demirtunc et al., Alhadas et al.
The average MPV value is 8.69 ± 1.43 fL in Diabetic group, and 7.44 ±0.68 fL in non – Diabetic (normal) group. MPV is significantly high in our study. The results of our study were similar to Kodiatte et al., Sharpe and Trinick et al, Hekimsoy et al, and Papanas et al. MPV is an indicator of average platelet size and its function.
Platelets become hyperreactive in Diabetes subjects that causes increase in activation, adhesion, and aggregation. Studies reported that larger platelets are younger, more active and more adhesive than smaller ones .They contain dense granules that secretes the prothromotic factors such as serotonin, β-thromboglobulin, platelet factor 4, and platelet-derived growth factor, that produces more thromboxane A2 and possess greater aggregability in response to ADP.19,20 Jones et al study reported that association of increased platelet volume and reduced platelet survival in Diabetic subjects.23 Therefore, larger platelets circulating in blood are mainly by increase in MPV, that predispose to thrombotic vascular complication in Diabetes patients.
In our study Table-3 shows that all platelet indices were increased in uncontrolled Diabetic patients when compared to the controlled Diabetic patients. This finding was similar to Kodiatte et al., and Zuberi et al., study. A high MPV is an important predictor for an increased risk for thrombosis and complications.
Several mechanisms have been proposed for an increased platelet activity in Diabetes due to hyperglycemia. The membrane proteins of platelet undergo a non – enzymatic glycation that reduces membrane fluidity and increase the platelet adhesion.10,25 An increase in calcium mobilisation from the storage pools and high level of intracellular calcium has been reported in Diabetes Mellitus patients. Intracellular free calcium is correlated with the reduction in membrane fluidity. Platelet activation is mediated by protein kinase C activation. Furthermore, due to hyperglycemia, osmotic swelling occurs that increase the platelet reactivity by glucose metabolites.
Platelet distribution width level in our study was increased in Diabetes when compared to non – Diabetic group. PDW was also significantly increased with poor glycemic control. Our findings were as similar as Jindal et al.,and Dalamaga et al study.25,27 Platelet activation causes changes in the morphology and pseudopodia formation. This difference in size and shape (discoid to spherical) leads to change in platelet distribution width.
In our study, plateletcrit (PCT) showed statistically significant difference (p<0.0001) between the two Diabetic group. Plateletcrit is higher in Diabetic groups than the normal group. Since the larger platelets are more reactive in Diabetic subjects, the platelet mass increases, thereby increasing PCT. Swaminathan et al study, found that PCT is high in the type 2 Diabetes Mellitus subjects (18). In khan et al study, PCT was higher in patients with hyperglycemia than the normoglycemia.
Table 1: Comparison of Physical Characteristics Between Controlled And Uncontrolled Diabetes Mellitus group
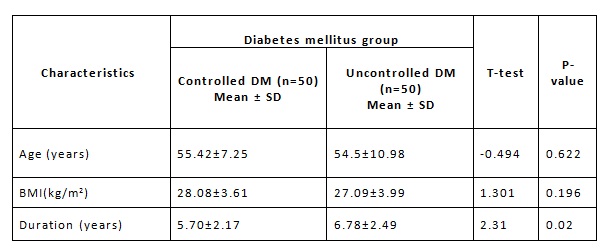
DM – Diabetes Mellitus, SD – Standard Deviation, BMI – Body Mass Index.
Table 2: Comparison of Blood Parameters Between Controlled and Uncontrolled Diabetes Mellitus group
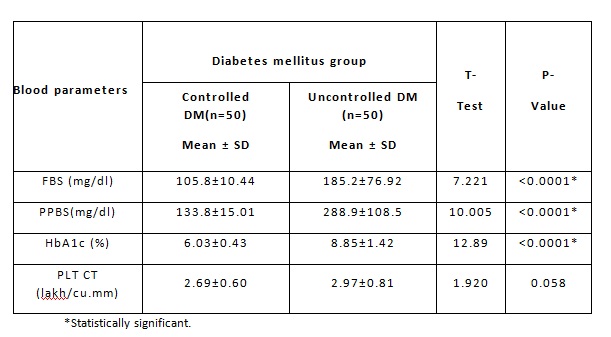
[Table -2]Among the Diabetic group, the FBS, PPBS and Hb A1c was higher in uncontrolled DM than the controlled DM subjects, which is statistically significant. The analysis shows that there was no significance between the platelet count of the two Diabetic groups.
Table 3: Platelet Indices in Diabetic Mellitus Subjects
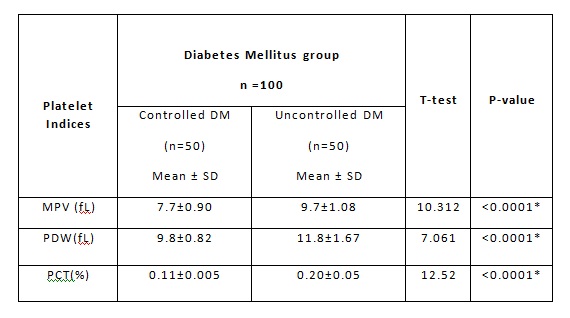
*Statistically significant. MPV: Mean platelet volume, PDW: Platelet
distribution width, PCT: Plateletcrit
Figure 1: Comparison Of Mean Platelet Volume between Controlled And Uncontrolled DiabetesMellitus Group
Figure 2: Comparison of Platelet Distribution Width between Controlled and Uncontrolled Diabetes Mellitus group
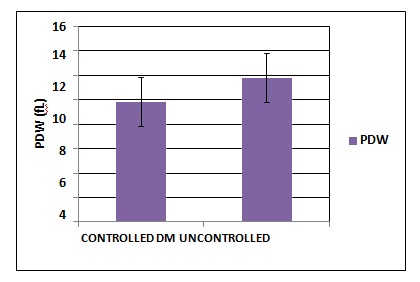
Figure 3: Comparison of Plateletcrit between Controlled and Uncontrolled Diabetes Mellitus group
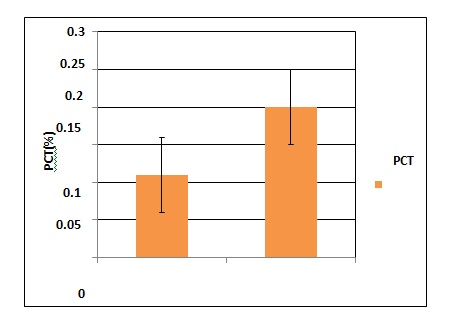
Table-3 and Figure 1,2,3 shows themean and standard deviation of the platelet indices values (MPV, PDW, PCT) of twoDiabeticgroups. Platelet indices between controlled and uncontrolled DM was statistically significant.
Table 4: Platetet Indices between Diabetic And Control Subjects
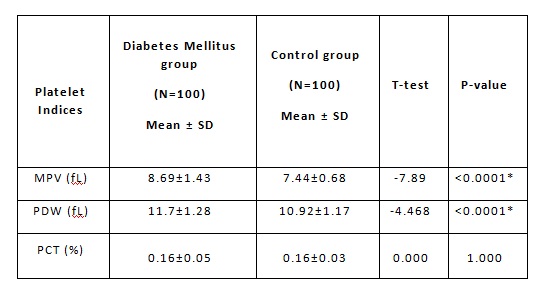
Figure 4: Comparison of Mean Platelet Volume between Diabetes Mellitus and Control group
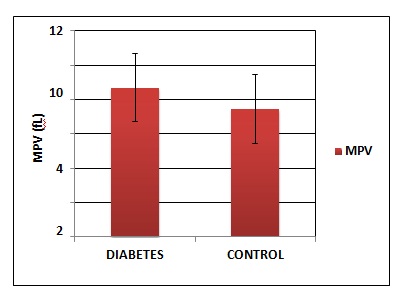
Figure 5: Comparison of Platelet Distribution Width between Diabetes Mellitus and Control group
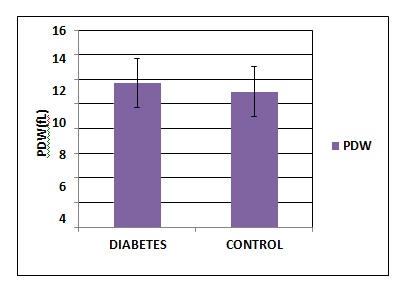
Figure 6: Comparison of Plateletcrit between Diabetes Mellitus and Control group
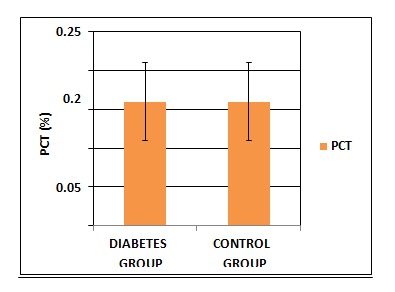
Table 4 and Figure 4,5,6 shows the comparison of the platelet indicesbetween the Diabetic group and control group. MPV and PDW shows statistical significance. The difference in plateletcrit was not significant between Diabetic and control group.
Conclusion: Our study found that hyperglycemia leads to platelet hyperactivity. Subjects with uncontrolled Diabetes Mellitus have an increase in morbidity and mortality. The control of glycemic status in each and every Diabetic individual can prevent the development of micro vascular and macro vascular complications. The regular treatment for Diabetes Mellitus is needed. Therefore, it improves the platelet activity and their functions. So, the platelet indices (MPV, PDW and PCT) could be used as a prognostic marker to monitor the platelet activation and progression of the complications in Diabetes Mellitus.
Acknowledgements: Nil.
Conflict of Interest: Nil.
References:
1. A. Fritsma G. Platelet Structure and Function. American Society for Clinical Laboratory Science. 2015 Apr 1;28:125–31.
2. Guyton and Hall. Textbook of medical physiology 11th ed.Philadelphia, PA : Saunders/Elsevier;c2006. Chapter 36,Hemostasis and Blood Coagulation; p. 457.
3. Vizioli L, Muscari S, Muscari A: The relationship of mean platelet volume with the risk and prognosis of cardiovascular diseases. Int J Clin Pract. 2009; 63:1509–1515.
4. Wiwanitkit V. Plateletcrit, mean platelet volume, platelet distribution width: its expected values and correlation with parallel red blood cell parameters. Clin ApplThrombHemost. 2004;10(2):175-178.
5. Yilmaz T, Yilmaz A. Relationship between Altered Platelet Morphological Parameters and Retinopathy in Patients with Type 2 Diabetes Mellitus. Journal of Ophthalmology. 2016 Apr 12;2016:1–5
6. Beckman JA, Creager MA, Libby P. Diabetes and atherosclerosis: epidemiology, pathophysiology, and management. JAMA. 2002 May 15;287(19):2570–81.
7. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010 Jan;87(1):4–14.
8. Cola C, Brugaletta S, Yuste VM, Campos B, Angiolillo DJ, Sabaté M. Diabetes mellitus: a prothrombotic state Implications for outcomes after coronary revascularization. Vasc Health Risk Manag. 2009;5:101–19.
9. Saboor M, Ilyas MS. Platelets structural, functional and metabolic alterations in diabetes mellitus. Pak J Physiol 2012;8(2).
10. Hekimsoy Z, Payzin B, Örnek T, Kandoğan G. Mean platelet volume in Type 2 diabetic patients. Journal of Diabetes and its Complications. 2004 May 1;18(3):173–6.
11. Biswal DP, Pradhan DP, Pradhan DD, Panda S. Evaluation Of Mean Platelet Volume (Mpv), As An Atherosclerotic Marker In Type 2 Diabetes Mellitus Patients. International Journal Of Scientific Research.2018 Sep 28;6(7).
12. EzgiCoşkunYenigün, Yenigün EC. Increased mean platelet volume in type 2 diabetes mellitus. Diclemedj. 2014 Mar 1;41(1):17–22.
13. American Diabetes Association Standards of Medical Care in Diabetes. Classification and diagnosis of diabetes. Diabetes Care 2017; 40 (Suppl. 1): S11-S24.
14. Kodiatte TA, Manikyam UK, Rao SB, Jagadish TM, Reddy M, Lingaiah HKM, et al. Mean platelet volume in type 2 diabetes mellitus. Journal of Laboratory Physicians. 2012 Jan 1;4(1):5.
15. Dayal A, Kothari S, Shah RJ, Patel SM. Mean Platelet Volume In Diabetes Mellitus Type II. 1. 2016 Dec 15;3(6):A567-572.
16. Papanas N, Symeonidis G, Maltezos E, Mavridis G, Karavageli E, Vosnakidis T, et al. Mean platelet volume in patients with type 2 diabetes mellitus. Platelets. 2004 Dec;15(8):475–8.
17. L SK, M R. Study of Platelet Indices in Type 2 Diabetic Patients and Its Correlation With Vascular Complications. 1. 2017 Oct 30;4(5):A591-598.
18. Swaminathan A, Amitkumar K, Ganapathy S, Ayyavoo S. Evaluation of mean platelet volume and other platelet parameters in subjects with Type-2 diabetes mellitus. Natl J Physiol Pharm Pharmacol. 2017;7(1):51.
19. Demirtunc R, Duman D, Basar M, Bilgi M, Teomete M, Garip T. The relationship between glycemic control and platelet activity in type 2 diabetes mellitus. Journal of Diabetes and its Complications. 2009 Mar 1;23(2):89–94.
20. Alhadas KR, Santos SN, Freitas MMS, Viana SMSA, Ribeiro LC, Costa MB, et al. Are platelet indices useful in the evaluation of type 2 diabetic patients? JornalBrasileiro de Patologia e Medicina Laboratorial. 2016 Apr;52(2):96–102.
21. Sharpe PC, Trinick T. Mean platelet volume in diabetes mellitus. Q J Med. 1993 Nov;86(11):739–42.
22. Gasparyan AY, Ayvazyan L, Mikhailidis DP, Kitas GD. Mean platelet volume: a link between thrombosis and inflammation? Curr Pharm Des. 2011;17(1):47–58.
23. Jones RL, Paradise C, Peterson CM. Platelet survival in patients with diabetes mellitus. Diabetes. 1981 Jun;30(6):486–9.
24. Zuberi B, Akhtar N, Afsar S. Comparison of mean platelet volume in patients with diabetes mellitus, impaired fasting glucose and non-diabetic subjects. Singapore medical journal. 2008 Mar 1;49:114–6.
25. Jindal S, Gupta S, Gupta R, Kakkar A, Singh HV, Gupta K et al. Platelet indices in diabetes mellitus: indicators of diabetes microvascular complications. Hematology 2011;16(2):86-9.
26. Schneider DJ. Factors Contributing to Increased Platelet Reactivity in People With Diabetes. Diabetes Care. 2009 Apr;32(4):525–7.
27. Dalamaga M, Karmaniolas K, Lekka A, Antonakos G, Papadavid E, et al. Platelet markers correlate with glycemic indices in diabetic, but not diabetic-myelodysplastic patients with normal platelet count. Dis Markers. 2010;29(1):55–61.
28. Khan SH, Ahmad SA. Platelet indices among subjects with and without diabetes mellitus and hypertension: a cross- sectional analysis at karachi, pakistan. Journal of Postgraduate Medical Institute (Peshawar – Pakistan). 2015 Dec 12;29(3).